
Legionella risk management for immunocompromised patients
- May 26
- 8 min read

Immunocompromised patient legionella risk management is not a niche concern. It sits at the intersection of clinical vulnerability and facility responsibility, and the stakes are significant. Almost half of all hospitalised Legionella patients are immunocompromised, and this group faces odds of 30-day mortality more than twice as high as immunocompetent counterparts. Add an ageing population, rising rates of immunosuppressive therapies, and increasingly complex water systems in healthcare buildings, and you have a problem that demands a more deliberate, layered response than standard Legionella protocols provide.
Table of Contents
Key takeaways
Point | Details |
Heightened mortality risk | Immunocompromised patients face over twice the odds of dying from Legionella pneumonia compared to other patients. |
Patient devices are blind spots | Items like water flossers brought in by patients can harbour Legionella and are rarely covered by standard water management plans. |
Dead legs and biofilms drive risk | Unmanaged dead legs and biofilm in pipework create protected Legionella reservoirs that chemical treatment alone cannot eliminate. |
Point-of-use filters are interim only | Filters protect vulnerable individuals at the tap but must be backed by permanent infrastructure improvements. |
Monitoring must be continuous | Testing frequency, temperature logging, and audit trails are non-negotiable in settings housing vulnerable patients. |
Why immunocompromised patients face distinct legionella risks
The clinical picture for immunocompromised patients diverges from the general population in ways that directly affect how facilities must respond. Because their immune systems cannot mount a typical inflammatory response, these patients may present with less severe initial symptoms despite carrying a disproportionate risk of rapid deterioration. That subtlety creates a diagnostic window that is both an opportunity and a danger.
The conditions that suppress immunity and increase susceptibility include solid organ and haematopoietic stem cell transplantation, haematological malignancies, HIV infection, long-term corticosteroid use, and biologic therapies used in autoimmune conditions. Each of these reduces the patient’s ability to clear Legionella pneumophila from the respiratory tract, making infection far more likely to progress to severe pneumonia. Treatment durations reflect this: immunocompromised patients require 21 days of antimicrobial therapy compared to 7 to 10 days for others.
On the environmental side, vulnerable patient legionella risk factors extend well beyond the main building water system. Consider the example published by the CDC: a patient developed nosocomial Legionella infection traced to a contaminated personal water flosser brought into hospital. The device had accumulated biofilm, aerosolised bacteria directly into the patient’s airway, and featured in no part of the facility’s water management plan. This is precisely the kind of gap that can exist even in otherwise compliant healthcare settings.
Facility design contributes its own set of vulnerabilities. Dead legs in water systems — sections of pipework where water sits stagnant at temperatures ideal for Legionella proliferation — create protected reservoirs that are difficult to detect without systematic assessment. Biofilm colonies inside piping add another layer of protection for the bacteria, shielding them from routine disinfection measures.
Pro Tip: When completing a risk assessment for a ward housing immunocompromised patients, map every water outlet including those rarely used, and specifically ask clinical staff whether patients bring in personal water-using devices. Document and restrict access where appropriate.
Building a water management plan for high-risk facilities
A water management plan (WMP) for a facility housing immunocompromised patients is not interchangeable with a standard commercial WMP. The regulatory baseline in the UK, set by HSE’s ACOP L8 and the associated Technical Guidance HTM 04-01 for healthcare premises, defines minimum requirements. But for facilities with vulnerable populations, those minimums are the starting point, not the finish line.
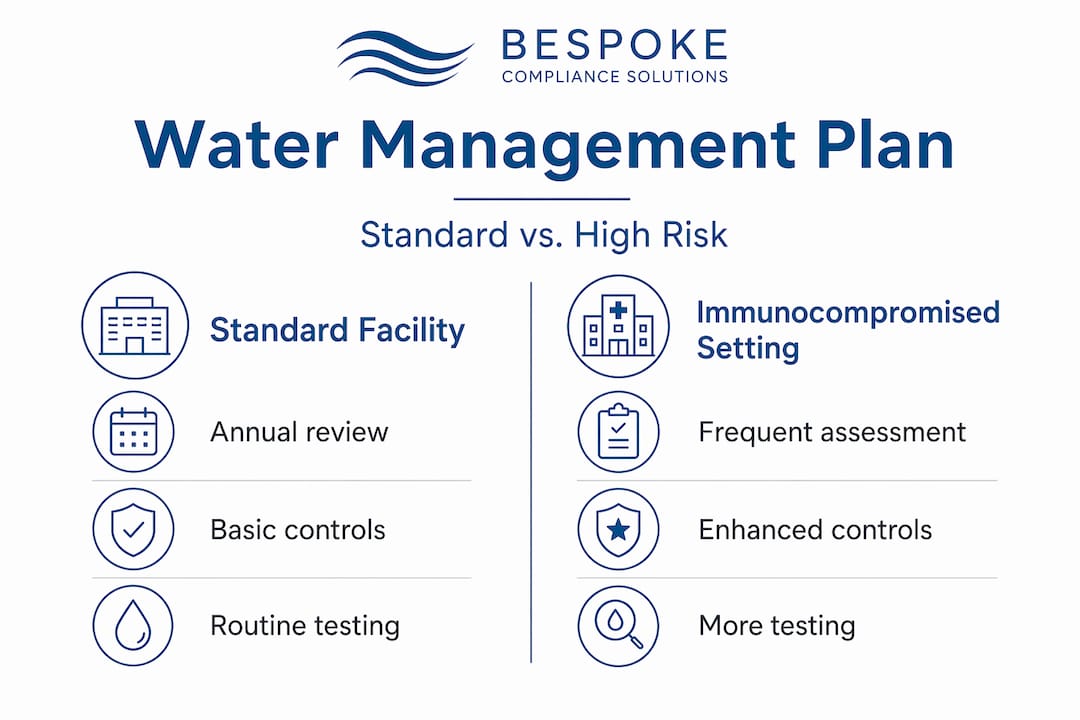
The table below shows how WMP elements should differ between standard and immunocompromised patient settings:
WMP component | Standard facility | Immunocompromised patient setting |
Risk assessment frequency | Every 2 years | Annually, or after any significant system change |
Water temperature targets | Cold below 20°C, hot above 50°C | Same targets, but monitored continuously rather than periodically |
Dead leg management | Identify and flush | Identify, eliminate where feasible, and flush weekly as a minimum |
Point-of-use filter use | Rarely required | Used as interim control on outlets serving highest-risk patients |
Patient device policy | Not typically addressed | Explicit policy restricting or managing patient-brought water devices |
Testing frequency | Quarterly as a minimum | Monthly or more frequently, aligned with heightened regulatory direction |
Regulatory direction is also tightening. New York City’s 2026 update mandates cooling tower testing every 31 days, a significant increase from previous quarterly requirements. While this is a US example, it signals a global pattern of intensifying scrutiny that UK healthcare facility managers should anticipate in domestic regulation as well.
Physical system design is the foundation on which every control programme rests. Temperature control is the primary defence, but it only works when the system architecture supports it. Dead legs allow water stagnation at temperatures within Legionella’s optimal growth range, typically between 25 and 45 degrees Celsius, meaning that no amount of chemical treatment will compensate for poor pipework design. Where elimination is not immediately feasible, weekly flushing protocols with documented records are the next best control.

Patient environment policy is an area many WMPs do not address explicitly. For facilities caring for immunocompromised individuals, this gap is a compliance and clinical risk. Any water management plan serving these settings should include a section on patient-owned devices with clear clinical guidance, procurement review, and ward-level communication to nursing staff.
Pro Tip: Engage your infection control team when drafting or revising your WMP. They can identify patient pathways and device use patterns that engineering teams would not ordinarily encounter during system surveys.
Executing legionella control measures effectively
Moving from a documented plan to effective daily execution is where many facilities fall short. The mechanics of control depend on integrating chemical, physical, and monitoring interventions rather than relying on any single approach.
Here is a practical sequence for executing controls in a high-risk patient setting:
Audit the water system to identify all dead legs, low-use outlets, and areas of thermal mixing. Reference your most recent legionella risk assessment findings and update the schematic.
Remove or flush dead legs on a documented schedule. Where dead legs cannot be removed immediately, weekly flushing with temperature verification is required.
Implement chemical dosing with the understanding that it is a supplementary control. Biofilm inside pipes neutralises chemical biocides unless physical cleaning and descaling are carried out first. Chemical treatment without prior physical intervention is not sufficient.
Install point-of-use filters on outlets serving immunocompromised patients as an interim measure. These filters provide a physical barrier at the point of delivery, but they require regular replacement and should not substitute for infrastructure repair. PoU filters are interim controls, not permanent solutions.
Deploy automated temperature monitoring on sentinel points across the system. Continuous data logging removes the human error factor from temperature verification and creates a real-time audit trail. Review temperature monitoring guidance to set appropriate thresholds and alert protocols.
Train all relevant staff including nursing, domestic, and estates teams on flushing protocols, the significance of patient-owned devices, and how to report concerns about water system anomalies.
Key operational controls to sustain on a continuous basis include:
Weekly flushing of all low-use outlets, recorded in a logbook with temperature readings
Monthly inspection of thermostatic mixing valves (TMVs) for condition and calibration
Immediate escalation protocol when outlet temperatures fall outside the control range
Quarterly review of point-of-use filter replacement records against installation dates
Annual review of the WMP in full, with a site walk to verify system schematics remain current
Monitoring, verification, and continuous improvement
Documentation is not bureaucracy. In the context of managing legionella risk for immunosuppressed patients, it is the mechanism by which you demonstrate ongoing control and identify drift before it becomes an incident.
Monitoring activity | Frequency | Action on exceedance |
Hot water temperature at sentinel points | Monthly | Investigate and re-test within 48 hours |
Cold water temperature at sentinel points | Monthly | Review insulation, check for heat gain sources |
Legionella water sampling (ward outlets) | Quarterly minimum | Immediate notification, flush and resample |
Cooling tower Legionella testing | Monthly (align with 2026 direction) | Shock dose, isolate if confirmed positive |
TMV service and calibration | Every 6 months | Replace or recalibrate, update service record |
Dead leg flushing and temperature check | Weekly | Escalate if temperature outside range, review elimination feasibility |
Interpreting results requires clinical as well as technical context. A low-level positive in a ward serving immunocompromised patients warrants a more aggressive response than the same result in a low-risk area. The infection control team should be notified immediately, and the decision about patient communication or environmental sampling expansion should be made jointly.
Effective surveillance also requires attention to antimicrobial resistance patterns. As resistance monitoring becomes more prominent in clinical guidance, facilities housing vulnerable patients should consider incorporating this into their water safety programme dialogue with microbiologists. This is an emerging area that will carry more weight in compliance conversations over the coming years.
Audit trails must support the full lifecycle of risk management: from initial assessment through control implementation, testing, corrective actions, and staff training records. If an incident occurs, a well-maintained logbook is both a defence and a diagnostic tool.
My perspective: what the guidance doesn’t prepare you for
I’ve reviewed and developed water management plans for a wide range of healthcare facilities, and the pattern I see most consistently is this: the physical water system gets attention, and patient-brought devices get none. The water flosser case from France is not an isolated curiosity. It reflects a structural blind spot in how risk management for immunosuppressed patients is framed. Standard WMPs are designed around fixed infrastructure. They do not account for the moving parts that patients introduce into the care environment.
The other thing I’ve learned is that compliance and actual control are not the same thing. A facility can have a signed-off WMP, a current risk assessment, and quarterly test results on file, and still have a ward with a dead leg that nobody has touched in two years. The paperwork says compliant. The pipework says otherwise. What bridges that gap is not more documentation. It’s a culture where estates, infection control, and clinical teams speak to each other regularly and treat Legionella as a shared clinical risk rather than an estates department checkbox.
My advice to facility managers working in healthcare: involve your infection control nurses in the WMP review process. They see patient behaviour that engineers don’t. And build a healthcare premises compliance framework that is genuinely multi-disciplinary, not one where water safety sits in isolation from clinical governance.
— Sammi
How Bespokecompliancesolutions supports healthcare legionella compliance
Protecting immunocompromised patients from Legionella exposure requires more than a generic compliance tick-box. Bespokecompliancesolutions works with healthcare facilities across the UK to develop and deliver genuinely bespoke water safety programmes. From system disinfection and flushing to the implementation of automated temperature monitoring and tailored logbook systems, every service is designed around your site’s specific risks and patient population. If you manage a facility serving vulnerable patients and want a compliance partner with real healthcare sector experience, explore our full range of legionella method of works and risk management services today.
FAQ
Why are immunocompromised patients at greater risk from Legionella?
Immunocompromised patients cannot clear Legionella pneumophila effectively, making infection more likely to progress to severe pneumonia. They face over twice the 30-day mortality risk compared to immunocompetent patients.
Are point-of-use filters enough to protect vulnerable patients?
No. PoU filters are an interim control that protect individuals at the point of delivery but must be supported by permanent infrastructure improvements to address the root cause of contamination risk.
What are the most overlooked legionella risk factors in healthcare settings?
Dead legs in pipework and patient-owned water devices are consistently underaddressed. A personal water flosser was linked to nosocomial Legionella infection in a case published by the CDC, highlighting how patient-brought items can fall entirely outside standard water management plans.
How often should Legionella testing occur in wards housing immunocompromised patients?
Quarterly water sampling is the accepted minimum, but high-risk patient areas warrant more frequent testing. Regulatory trends, including NYC’s 2026 mandate for monthly cooling tower testing, reflect a broader shift toward increased testing frequency for vulnerable population settings.
Does chemical treatment alone control Legionella in healthcare water systems?
No. Chemical biocides are neutralised by biofilm unless physical cleaning and descaling are carried out first. Effective control requires both physical and chemical interventions applied in the correct sequence.
Recommended
Comments